In the weeks, and sometimes months, after the amputation of a limb, the pain can be overwhelming. It may not be the physical pain alone that consumes the patient – the mental ramifications of losing part of the body can throw people for a loop.
Opioids are a class of drugs commonly prescribed to many patients following any type of surgery. From the National Institute on Drug Abuse: “Opioid pain relievers are generally safe when taken for a short time and as prescribed by a doctor, but because they produce euphoria in addition to pain relief, they can be misused (taken in a different way or in a larger quantity than prescribed, or taken without a doctor’s prescription).”
In the first weeks after surgery, opioids may be one of the only ways that the patient can find relief. In addition, control of acute pain can help keep chronic pain from forming: “Acute pain progresses into chronic pain when repeated or continuous nerve stimulation precipitates a series of altered pain pathways, resulting in central sensitization and impaired central nervous system mechanisms.”1 If the patient’s brain does not create those pain pathways in their brain, they’re less likely to experience chronic pain.
In time, and, when possible, the opioids that the patient is taking generally should, with the supervision of a doctor, be tapered off. To quote the National Institute on Drug Abuse again: “Regular use—even as prescribed by a doctor—can lead to dependence and, when misused, opioid pain relievers can lead to addiction, overdose incidents, and deaths.” There are other pain medications that can be prescribed for longer term pain management – patients should ask their doctor about those options.
But what else can be done to deal with both the physical pain of upper limb amputation and the mental anguish that goes along with limb loss?
Basic Approaches
Sleep, diet and exercise. We all know how important these three cornerstones are to our everyday lives, but they’re worth re-evaluating in the months following an amputation. Healing takes time and self-care.
Keep in mind that everyone’s experience of pain is different. Even amongst people who have had similar reasons for an amputation and similar amputation levels, the perception of pain can be felt differently by each individual. So as the patient is assessing their pain management needs, it’s best to think about what they need and not worry about how other people are managing.
Relaxation and Meditation
Even if the patient has never meditated before in their life, it can be easy to get started. Deep breathing is a simple place to begin. If the patient feels their anxiety easing up, they can further explore meditation options.
Graded Motor Imagery and Mirror Therapy
Graded Motor Imagery is a non-invasive treatment option that can help decrease phantom limb pain (and improve myoelectric prosthetic control). There are three steps to it: laterality reconstruction, which is a training program that targets the neurologic connections between the brain and the missing limb; motor imagery, which involves imagining movement of the affected limb; and mirror therapy, wherein the patient views the unaffected limb in a mirror, while keeping the residual limb out of sight – these actions can cause the brain to “re-think” the pain response. Graded Motor Imagery should be performed with the initial guidance of a clinical therapy specialist. If you are looking for a therapist to work with, please contact us.
The Wellness Inventory
Recovering from an amputation requires not only managing pain but addressing other important needs as well. Our Arm Dynamics patients are encouraged to complete the Wellness Inventory, a confidential, written assessment that can help us understand their individual challenges and connect them with counseling, if needed.
Addressing Acute Issues
Problems like overuse issues or neuromas can be diagnosed by the care team, consisting of the patient’s doctor, prosthetist and therapist. While the solutions may take work on the part of the patient, or create a need for medication or steroid injections, it can be possible to make the pain disappear, or nearly so. Patients should also be aware if their prosthesis is the cause of ongoing pain. Some patients are told that it’s normal for the socket to be uncomfortable. But a socket that’s fit correctly doesn’t cause pain or make callouses on the limb. All our Arm Dynamics prosthetists and therapists are upper-limb prosthetic specialists and can help patients get into a custom-fit silicone socket that relieves pain, feels lighter and keeps the residual limb cooler.
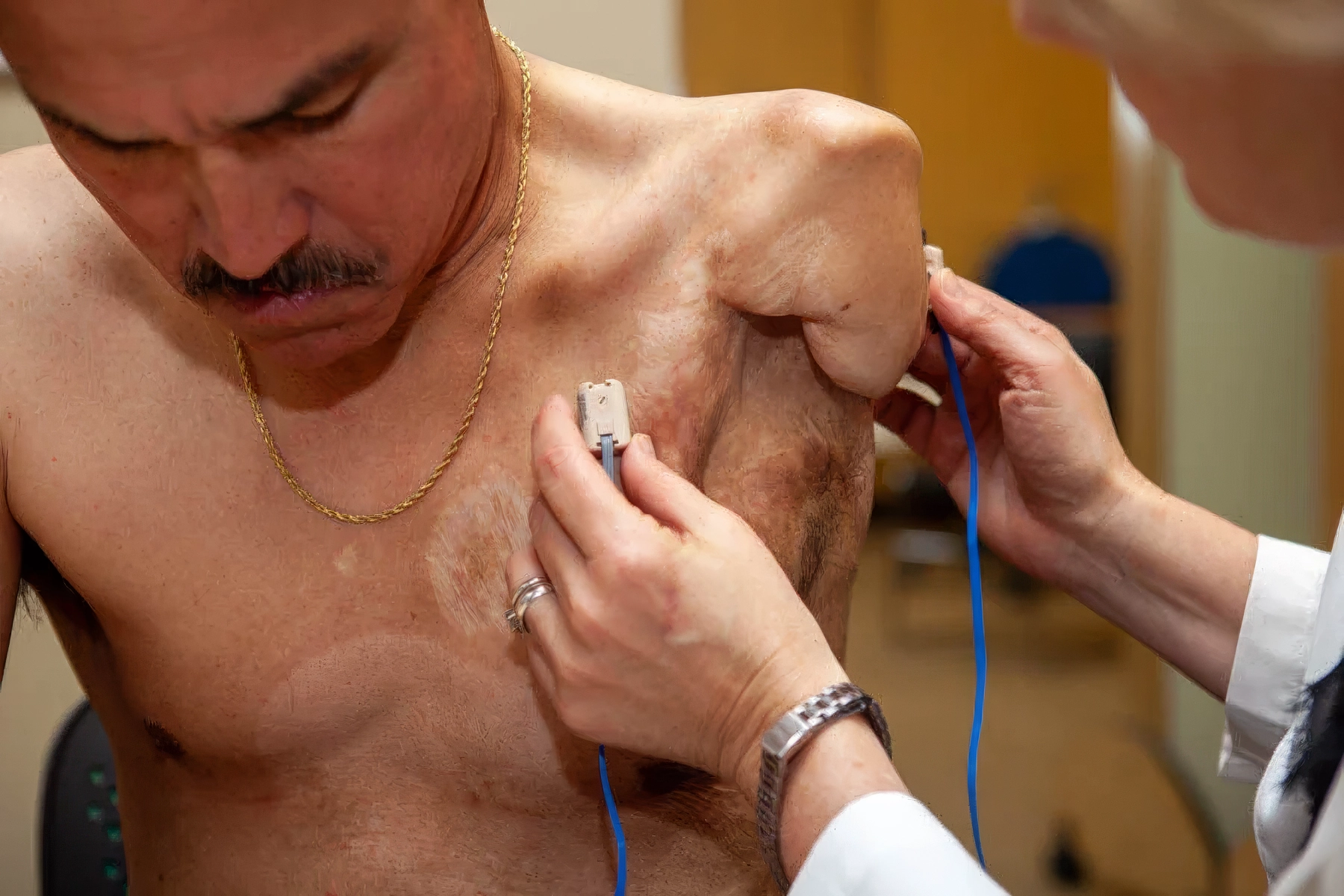
Surgery
In some cases, like stubborn neuromas or persistent phantom limb pain, surgery may be the solution that a doctor recommends. Targeted Muscle Reinnervation (TMR) is a surgical procedure where the surgeon “reassigns” nerves that once controlled hand or arm muscles on the residual limb or chest. Giving a severed nerve a new “job” helps prevent neuroma growth and normalizes the nerve signals that are sent to the brain, thereby reducing pain signals. While this surgery is often performed to allow for better control of myoelectric devices, we have had our patients tell us that it is worth it for the pain relief alone.
We recognize the importance of patients having access to all forms of pain relief, under the supervision of their doctor, and we also want to make sure that amputees are aware of the alternatives to opioids. Would you like to learn more about how our clinical team helps patients heal and move past their pain so they can get back to their work and home lives? Please reach out. Do you have an experience with any of the pain relief options above? Please let us know in the comments below.
References
1: How Does Acute Pain Become Chronic? By Gloria Arminio Berlinski, MS
Reviewed by Christopher Gharibo, MD, Medical Director of Pain Medicine, NYU Langone Medical Center Hospital for Joint Diseases, New York, NY
MedPage Today
https://www.medpagetoday.com/resource-centers/pain-management/does-acute-pain-become-chronic/1040






%20President%20and%20Senior%20Clinical%20Director.jpg?width=600&height=600&name=John%20M.%20Miguelez%2c%20CP%2c%20FAAOP(D)%20President%20and%20Senior%20Clinical%20Director.jpg)








Comments (2)